Proposed CY 2027 HH PPS Payment Update Rule Posted
The proposed Calendar Year 2027 Home Health Prospective Payment System (HH PPS) Rate Update; Requirements for the HH Quality Reporting Program and the Expanded HH Value-Based Purchasing Model; Medicare Provider Enrollment, Durable Medical Equipment (DME), and DME, Prosthetics, Orthotics, and Supplies (DMEPOS) Policies was posted on the Federal Register Public Inspection desk on 7/1/2026.
Please note: there are items in this rule that apply to Medicare-certified hospice providers.
Providers are strongly encouraged to review the rule in its entirety as this is only a summary of the content and to send comments to CMS by August 31, 2026. Here are the highlights of the final rule.
Payment Update
CMS is proposing an overall 2.4% increase in Medicare payments to home health agencies for CY 2027, representing approximately $420 million in additional payments across the industry. The increase is driven by a 2.1% annual payment update and a 0.3% increase resulting from updates to outlier payment calculations.
CMS also proposes continuing the 3.0% temporary reduction designed to recoup overpayments associated with the implementation of the Patient-Driven Groupings Model (PDGM). This reduction is expected to recover approximately $500 million in 2027.
CMS does not propose any new permanent behavioral adjustment, noting that most PDGM-related behavioral changes had already stabilized by 2022.
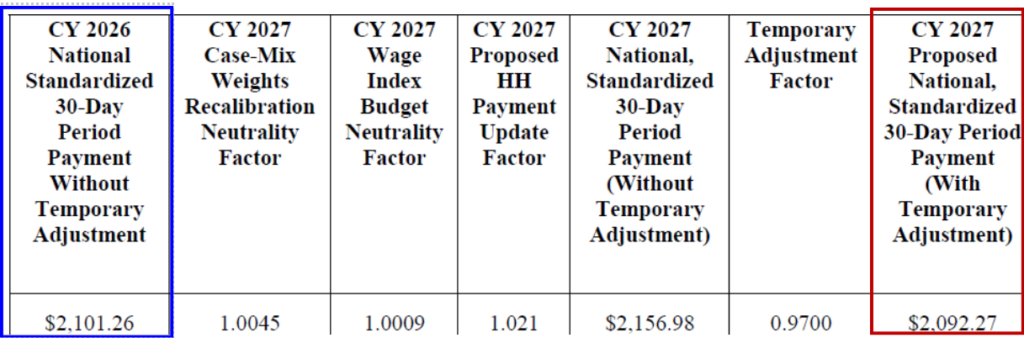
Proposed CY 2027 National, Standardized 30-Day Period Payment Amount
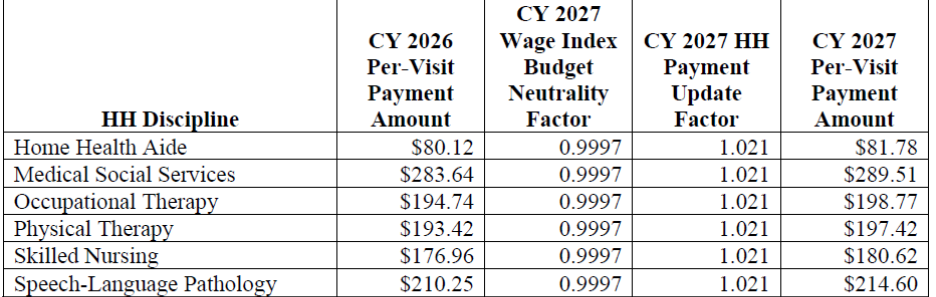
The proposed CY 2027 national per-visit rates for HHAs that submit the required quality data are updated by the proposed CY 2027 home health payment update percentage of 2.1%.
Proposed CY 2027 National Per-Visit Payment Amounts
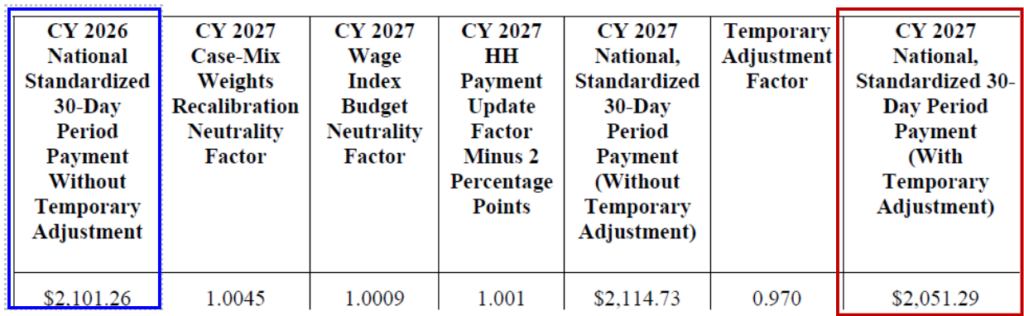
For HHAs that do not submit the required quality data for CY 2027, the proposed home health payment update percentage is 0.1 percent (2.1 percent minus 2 percentage points).
Proposed CY 2027 National, Standardized 30-Day Period Payment Amount For HHAs That Do Not Submit The Quality Data
Proposed CY 2027 National Per-Visit Payment Amounts For HHAs That Do Not Submit The Required Quality Data

Opportunity for comment: CMS invites public comments on the proposed CY 2027 home health market basket percentage increase and productivity adjustment, on the proposals to not apply a permanent adjustment and to apply the -3.0 percent temporary adjustment to the CY 2027 home health base payment rate, and on proposed updates to the LUPA thresholds for CY 2027.
Request for Information – Home Health Specific Wage Index
CMS acknowledges that the hospital wage index may not accurately reflect the labor costs faced by home health agencies. As a result, the agency is seeking feedback on whether alternative data sources could be used to create a wage index that more closely reflects the home health workforce and home health operating environment.
Specifically, CMS is considering whether future wage index calculations could incorporate:
- Bureau of Labor Statistics (BLS) occupation-level wage data.
- Home health cost report data.
- Other methodologies that better capture local labor costs for home health providers.
For CY 2027, CMS proposes to:
- Continue using the hospital wage index as the basis for home health payments
- Continue applying the existing 5% cap on annual wage index decreases, which protects agencies from significant year-over-year payment reductions due to wage index changes
- The proposed HH PPS wage index file applicable for CY 2027 (January 1, 2027, through December 31, 2027) is available on the CMS website at https://www.cms.gov/medicare/enrollment-renewal/providers-suppliers/home-health-agencycenter.
Opportunity for comment: CMS solicits comments on whether we should consider using alternative data sources to construct an HHA specific wage index for potential use in future years. CMS seeks feedback to understand the potential advantages and limitations of using alternative data sources, such as BLS data and home health Medicare cost reports, as well as other methodologies that stakeholders believe could appropriately reflect the geographic variation in labor costs for HHAs. We also seek feedback on the unique considerations applicable to HHAs that should inform how CMS considers the potential use of alternative data sources.
Annual PDGM Recalibration Continues
As in previous years, CMS proposes routine recalibration of several payment system components using more recent claims data. Updates would affect:
- Case-mix weights
- Functional impairment levels
- Low Utilization Payment Adjustment (LUPA) thresholds
- Comorbidity adjustment categories
- Per-visit payment rates
- Short-stay add-on payment factors
These annual adjustments are intended to ensure that reimbursement more accurately reflects contemporary utilization patterns and patient characteristics.
CMS proposes to use the same methodology previously finalized to update the functional impairment levels for CY 2027. The proposed updated OASIS functional points table and the table of functional impairment levels by clinical group for CY 2027 are listed in tables 19 and 20, respectively.
Opportunity for comment: CMS solicits public comments on the proposed updates to the functional points and the functional impairment levels by clinical group and proposed updates to the low comorbidity adjustment subgroups and the high comorbidity adjustment interactions for CY 2027. CMS also invites public comments on the CY 2027 proposed case-mix weights and proposed case-mix weight budget neutrality factor.
Home Health Quality Reporting Program Updates
CMS proposes changes that would affect both data reporting timelines and the long-term structure of home health quality measurement. These proposals are intended to provide greater consistency for providers while supporting CMS’s broader quality strategy.
- Alignment of OASIS and HHCAHPS Reporting Periods
- Proposal made to align the reporting periods for the Outcome and Assessment Information Set (OASIS) and the Home Health Care Consumer Assessment of Healthcare Providers and Systems (HHCAHPS) survey with the calendar year.
- Currently, providers often manage multiple reporting cycles and timelines across quality programs. By synchronizing reporting schedules, CMS seeks to create a more streamlined process that may reduce administrative burden and make performance monitoring more consistent across reporting programs.
- For home health agencies, this change could simplify quality oversight activities by creating a more predictable annual reporting cycle and improving the ability to analyze organization-wide quality performance trends.
- Shorter OASIS Submission Deadlines
- Proposal made to shorten the deadline for OASIS data submission. Specifically, OASIS data would need to be submitted by the 15th day of the second month following the reporting quarter.
Proposed Data Collection Timeframe And Data Submission Deadlines For Oasis Assessment Data Affecting The Cy 2029 Payment Determination

- This proposal reflects CMS’s interest in obtaining quality data more quickly to support performance monitoring, public reporting, and future payment initiatives.
Opportunity for comment: CMS invites comment on this proposal to require that HHAs complete their data submissions and make corrections to their OASIS assessment data where necessary no later than the 15th day of the second month after the end of the calendar quarter beginning with the CY 2027 HH QRP.
- HH QRP Measure Concepts Under Consideration for Future Years – Request for Information (RFI)
- CMS seeks input on the importance, relevance, appropriateness, and applicability of the quality measure concepts related to advanced care planning.
- No new measures are proposed in the proposed rule.
Expanded HHVBP Model – Home Health Value-Based Purchasing
- CMS is not proposing any changes for the expanded HHVBP Model.
- They included a summary of the Model with context relevant to potential alignment between the HH QRP and the expanded HHVBP Model.
Medicare Provider Enrollment
CMS is proposing several provider enrollment provisions. The provisions would affect any providers and suppliers participating in the Medicare program. These changes would help reduce improper Medicare payments and protect beneficiaries. Proposals include but are not limited to:
- Expanded Authority to Deny or Revoke Enrollment – CMS proposes broader authority to deny or revoke Medicare enrollment for providers and suppliers that present elevated program integrity risks. The proposal would expand CMS’s ability to act based on certain misdemeanor conduct and patterns of activity associated with high-risk practice locations.
- Adding or Expanding Bases for Revocation or Denial — CMS is proposing to add several new grounds for revocation or denial of enrollment and to expand some of our existing grounds. Among these proposals are the following:
- Change in Majority Ownership — Hospices; HHAs; and suppliers of durable medical equipment, prosthetics, orthotics, and supplies (DMEPOS) must reenroll in Medicare as a new provider and undergo a survey/accreditation if they experience certain changes in majority ownership. CMS proposes to deny or revoke enrollment if this requirement is violated.
- Program or License Suspension/Termination — CMS currently may deny or revoke enrollment if a provider: (1) has a suspended/revoked license in another state; or (2) is suspended/revoked from Medicaid or another federal healthcare program. The agency proposes expanding this to include similar suspensions/revocations involving the provider’s owners or managing employees/organizations.
The proposed revocation/denial authorities would address situations noted by CMS as involving provider noncompliance and fraud, waste, and abuse. They also would allow the agency to target improper activity by those who own or operate providers.
- Definition updates – Proposal to update the following definitions:
| Definition | Proposed Change |
| Managing Employee | Expanded to explicitly include medical directors (beyond hospice and SNFs), clinical directors, departmental heads, supervising physicians, nursing directors, alternate administrators, and other clinical personnel who exercise operational or managerial control. |
| Final Adverse Action | Expanded to include certain misdemeanor convictions related to sexual assault or financial misconduct occurring within the previous 10 years. |
| Operational | Revised to establish more detailed requirements regarding practice locations, patient accessibility, staffing, equipment, visibility to beneficiaries, policies, records, and readiness to furnish services and submit claims. |
| Affiliation | Expanded to encompass additional operational, managerial, business, financial, marketing, fulfillment, and beneficiary relationships between entities. |
CMS is proposing new and more detailed requirements tied to what constitutes a legitimate practice location through revisions to the definition of “operational” and related enrollment requirements. Rather than simply having an address on file, providers and suppliers would be expected to maintain a qualified practice location that demonstrates actual operational capability.
| Proposed Requirement | Description |
| Qualified Practice Location | Providers must operate from a legitimate location capable of furnishing healthcare services. |
| Patient Accessibility | The location must be accessible to patients and free of safety hazards. Accessibility includes compliance with applicable ADA requirements and equivalent state or local laws. |
| Open and Available to the Public | The provider must be open for the purpose of furnishing healthcare-related services and maintain business hours sufficient to regularly serve patients. |
| Public Visibility | Medicare beneficiaries must be able to identify and locate the provider using publicly available information. |
| Permanent Signage | CMS proposes a new requirement that providers maintain a permanent visible sign and post hours of operation. If located within a building complex, signage must be visible at the main entrance or the provider’s entrance. |
| Adequate Staffing and Resources | The location must be properly staffed, equipped, stocked, and capable of furnishing the services for which the provider is enrolled. |
| Operational Records and Policies | Providers must maintain appropriate operational policies, patient care procedures, safety policies, and medical records. |
- Hospice Medical Directors and Administrators (§ 424.530(a)(20)) – CMS proposes a new Medicare enrollment denial authority specifically targeted at hospice medical directors and administrators as part of its broader hospice program integrity efforts. CMS would be permitted to deny a hospice’s Medicare enrollment application if any of the following conditions exist:
- Medical Director Oversight Concerns
- A hospice could be denied enrollment if its medical director:
- Serves as the medical director for multiple other hospices.
- Is located so far from the hospice (for example, in another state) that CMS determines the individual cannot realistically perform all required medical director responsibilities.
- Does not hold an active physician license in the state where they practice.
- Administrator Oversight Concerns – A hospice could also be denied enrollment if its administrator:
- Serves as administrator for multiple hospices.
- Is located at such a distance from the hospice that CMS determines they cannot realistically carry out their required administrative responsibilities.
- Medical Director Oversight Concerns
Section 424.530(a)(20) would not: (1) formally prohibit medical directors and administrators from serving at more than one hospice; or (2) change hospice CoPs or other hospice policies in 42 CFR part 418. It would simply help CMS address situations where the hospice’s prospective enrollment raises the program integrity concerns.
- CMS Enrollment Form Revisions – CMS also announced their intention to revise the following provider enrollment application ns to require all suppliers completing these forms to identify whether any organizations disclosed thereon are PECs or REITs:
- Form CMS-855B (Medicare Enrollment Application – Clinics/Group Practices and Certain Other Suppliers; OMB Control No. 0938-1377).
- Form CMS-855S (Medicare Enrollment Application – Durable Medical Equipment, Prosthetics, Orthotics, and Supplies (DMEPOS) Suppliers; OMB Control No. 0938-1056).
- Form CMS-20134 (Medicare Diabetes Prevention Program (MDPP) Suppliers).
They state intended form revisions would not involve regulatory changes.
Opportunity for comment: CMS solicits and welcomes comments on all the proposed provider enrollment provisions.
Program Integrity
- Expanded Enrollment Screening and Revocation Authorities – CMS proposes to strengthen its ability to deny or revoke provider and supplier enrollment when program integrity concerns exist. The proposal expands CMS’s authority to address situations involving high-risk business practices, questionable operational arrangements, and certain misdemeanor offenses that may indicate an increased risk to the Medicare program.
- Greater Oversight of Ownership and Control – The proposal places increased emphasis on transparency regarding ownership, management, and organizational control. CMS seeks additional safeguards around ownership changes and enhanced scrutiny of individuals who exercise significant influence over provider operations, including administrators, managing employees, and hospice medical directors.
- Enhanced Physical Location Requirements – To combat the use of shell companies and fraudulent enrollment practices, CMS proposes requiring providers and suppliers to maintain a bona fide operational presence at their enrolled practice location. This includes expectations regarding physical accessibility and visible business identification, such as signage (there are signage exceptions detailed in the rule). https://chap1275-my.sharepoint.com/personal/jennifer_kennedy_chapinc_org/Documents/Microsoft Copilot Chat Files/CY 2027 payment update-NPRM.pdf
- Reduced Timeframe for Claims Submission Following Revocation – The proposal would shorten the period during which revoked providers can submit Medicare claims from 60 days to 15 days. CMS believes this change would reduce opportunities for inappropriate billing after enrollment termination actions have occurred.
- Increased Oversight of Recent Changes of Ownership – CMS proposes closer review of providers that undergo ownership changes within 36 months of enrollment. Frequent or rapid ownership transfers have been identified as potential indicators of program integrity risk, and CMS seeks greater ability to monitor these situations.
DMEPOS and Infusion Coverage
The proposed rule also contains several updates affecting durable medical equipment (DME) and infusion therapy coverage.
- CMS is proposing to simplify Medicare requirements for replacing durable medical equipment, prosthetics, orthotics, and supplies (DMEPOS). Under the proposal, providers would still be required to obtain a new physician order when replacing a DMEPOS item, but they would no longer need to obtain a new face-to-face evaluation if the replacement item falls under the same HCPCS code as the original item.
However, if a beneficiary’s clinical condition changes and a different type of equipment is needed—resulting in a different HCPCS code—a new face-to-face examination would still be required under existing Medicare rules.
CMS states that requiring another clinical evaluation when the patient is simply replacing the same type of equipment is often redundant and unnecessarily burdensome because the beneficiary’s need for that item has already been established.
The proposal:
- Does not eliminate the requirement for a new order.
- Does not change existing Medicare coverage requirements.
- Does not supersede national or local coverage determinations (NCDs or LCDs).
- Expanded Coverage for Certain External Infusion Pumps and Home Infusion Drugs — CMS proposes to amend the DME definition at 42 CFR 414.202 to implement Section 6222(a) of the Consolidated Appropriations Act, 2026. The proposal would expand DME benefit coverage to certain external infusion pumps, associated home infusion drugs, and related supplies that may not otherwise meet the current “appropriate for use in the home” standard, provided specific safeguards are met. The proposed effective date is April 1, 2027.
- Under the proposal, coverage would apply when all the following criteria are satisfied:
- The FDA-approved prescribing information for the home infusion drug indicates that the drug should be administered by, or under the supervision of, a healthcare professional.
- A qualified home infusion therapy supplier administers or supervises administration of the drug or biological safely and effectively in the patient’s home.
- The prescribing information indicates that the drug should be infused at least 12 times per year.
- Infusion occurs intravenously or subcutaneously.
- The infusion rate is one that CMS determines requires use of an external infusion pump.
To support safe home infusion, CMS proposes that the supervising healthcare professional may be a registered nurse, clinical nurse specialist, nurse practitioner, physician assistant, or physician. CMS also proposes interpreting the “at least 12 times per year” requirement to mean at least once per month, reflecting typical drug dosing schedules.
Opportunity for comment: CMS solicits comments on this proposal.
- Country-of-Origin Reporting Requirements – CMS proposes requiring suppliers participating in the DMEPOS Competitive Bidding Program (CBP) to report the country of origin for designated lead items furnished to Medicare beneficiaries. CMS describes this proposal as a transparency initiative intended to provide greater visibility into where certain DMEPOS products are manufactured.
- Enhanced Fraud, Waste, and Abuse Reporting – CMS proposes in new § 424.58(c)(1)(xxiii)(N) that a DMEPOS accreditation organization must agree to notify CMS in writing (and, if applicable, law enforcement) of suspected fraud, waste, and abuse — consistent with the AO’s CMS-approved definitions of those terms — within 3 calendar days of the date on which the AO determines that fraud, waste, or abuse may have occurred.
Hospice Reactivations
CMS proposes additional requirements for hospices seeking to reactivate Medicare billing privileges after a period of deactivation, reflecting the agency’s broader effort to strengthen enrollment oversight and safeguard the Medicare program.
- CMS proposes hospices seeking reactivation may be required to undergo additional survey or accreditation activities as part of the reactivation process.
- CMS believes these reviews would help confirm that providers remain operational and compliant with Medicare requirements before they resume billing.
Opportunity for comment: CMS solicits comments on this proposal.
Palliative Care Services as Home Health Services
The rule includes a discussion clarifying that palliative care services can be provided and covered under the Medicare home health benefit when a beneficiary meets home health eligibility requirements and the services are ordered by an allowed practitioner. CMS emphasizes that palliative care should not be viewed as synonymous with hospice care and that beneficiaries do not need to be terminally ill to receive palliative care services under home health.
CMS explicitly states that beneficiaries who qualify for Medicare home health services may receive palliative care under the home health benefit. The agency notes that patients do not need to forgo life-prolonging treatments, be terminally ill, or demonstrate rehabilitation potential to qualify for skilled services. Even when full recovery is unlikely, skilled services may be reasonable and necessary to prevent deterioration or maintain current function.
CMS believes that the regulatory definition of palliative care aligns closely with the services already covered under the Medicare home health benefit. Palliative care is defined as patient- and family-centered care that focuses on improving quality of life through the anticipation, prevention, and treatment of suffering while addressing physical, emotional, social, spiritual, and informational needs. The agency notes that many traditional home health services inherently support palliative care goals, including:
- Skilled nursing services
- Physical therapy
- Occupational therapy
- Speech-language pathology
- Medical social services
- Home health aide services and medical supplies
CMS highlights skilled nursing as a critical component of home-based palliative care. Skilled nursing services may include:
- Advanced symptom management
- Pain control
- Management of nausea and vomiting
- Treatment of anxiety and depression
- Respiratory symptom management
- Medication monitoring and adjustment in coordination with practitioners
Patients with multiple chronic conditions, complex medication regimens, and functional limitations may require ongoing skilled observation and medication management that can be provided through the home health benefit.
CMS emphasizes that palliative care extends beyond nursing services and benefits from a multidisciplinary approach:
Medical Social Services
- Advance care planning discussions
- Hospice transition counseling when appropriate
- Emotional and psychosocial support
- Caregiver support and resource referrals
Physical Therapy
- Mobility support
- Pain management techniques
- Safe transfer training
- Functional maintenance strategies
Occupational Therapy
- Adaptation of activities of daily living
- Environmental modifications
- Strategies to maintain independence and safety
Speech-Language Pathology
- Support for eating and swallowing
- Communication assistance
- Facilitation of patient decision-making and care planning
Documentation Expectations
CMS stresses that palliative care services must meet the same documentation standards as any other skilled home health service. Clinical records should clearly demonstrate:
- The patient’s care needs and goals
- Why skilled services are necessary
- Interventions provided
- Progress toward goals outlined in the plan of care
- Ongoing need for medication management, assessment, teaching, and observation
Importantly, CMS notes that a terminal diagnosis alone does not determine coverage. Coverage depends on whether the services require the skills of qualified clinicians and are properly documented.
CMS plans on adding additional palliative care examples of skilled care to the Benefit Policy Manual following the publication of the CY 2027 HH PPS final rule to support our goal of encouraging community-based palliative care services, particularly under the Medicare home health benefit.
Opportunity for comment: CMS solicits comments on any concerns or suggestions regarding reaching this goal.
Review the proposed rule on the Federal Register Public Inspection desk
https://public-inspection.federalregister.gov/2026-13602.pdf
For further information, see the CMS Fact Sheet of the HHA proposed rule https://www.cms.gov/newsroom/fact-sheets/calendar-year-cy-2027-home-health-prospective-payment-system-proposed-rule-fact-sheet-cms-1844-p
Questions about the content of this rule? Contact CHAP